Other Name: Radial sensory nerve.
Key Points:
- Patient complaints of pain at the posterior and lateral aspect of the forearm, wrist, and hand require examination of this nerve.
- This nerve is classically known as a ‘bad actor’ due to its delicate nature to injury. A minor injury can result in significant neuropathic pain. Any invasive procedure that occurs within the area that the nerve courses, the surgeon should take extreme caution and preferably under tourniquet to allow visualization and protection of this nerve and its branches.
Sensory Innervation:
- Provides sensation to the posterior and radial cutaneous aspect of the arm.
- Originates from roots C6, C7, C8 and branches from the radial nerve.


EXAMINATION
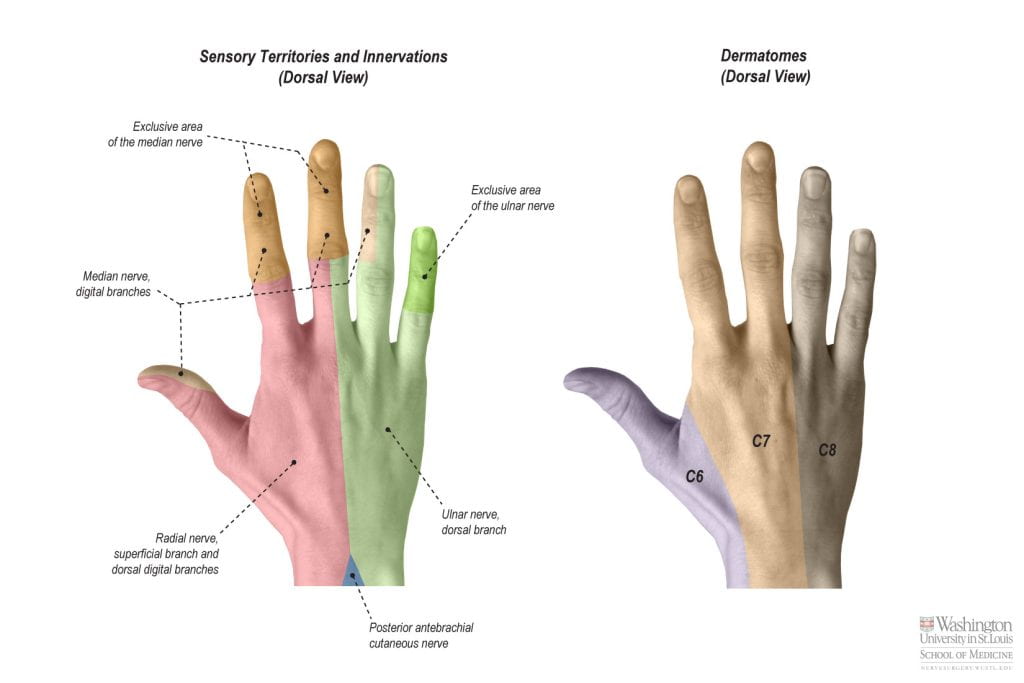
Sensory examination includes testing the dorsal radial aspect of the distal forearm/wrist and hand innervated by the superficial branch of the radial nerve.
Sensory Examination:
- Ask patients to draw area of diminished sensation/numbness on a hand diagram.
- Test the skin along the dorsal radial aspect of the distal forearm/wrist and hand for reduced/absent sensation by use of light touch or other sensory examination modalities.
Clinical Relevance:
- Provides sensation to the dorsal radial aspect of the distal forearm/wrist and hand.
- Wartenberg’s Syndrome – The superficial radial sensory nerve can be entrapped between the brachioradialis tendon and the extensor carpi radialis longus tendon as it exits the deeper compartments and become superficial.
- This nerve is delicate in nature and can be easily injured during procedures that occur in the area that the nerve courses. De Quervain’s release being one of them.
- During examination, differentiating an injury to the LABC nerve versus the superficial radial sensory nerve can be challenging due to the sensory territories overlapping within the distal forearm and wrist.
- Eliciting a Tinel’s sign over the individual nerves as they course superficially can help distinguish between them:
- Lateral Antebrachial Cutaneous Nerve: A Tinel’s test over the antecubital fossa just medial to the brachioradialis muscle.
- Radial Sensory Nerve: A Tinel’s test over the area where the radial sensory nerve courses superficially between the tendons of the brachioradialis and extensor carpi radialis longus muscles.
- A diagnostic block to either nerve to see if this alleviates symptoms may also be helpful in determining further interventions.
Adjacent Sensory Distribution:
PROXIMAL/MEDIAL – Posterior antebrachial cutaneous nerve.
PROXIMAL/LATERAL – Lateral antebrachial cutaneous nerve. *Note that 25% of the time, this nerve completely overlaps the superficial branch of the radial nerve sensory distribution; the remainder of the time, there is some degree of subtotal overlap with the radial sensory nerve territory.
MEDIAL – Dorsal cutaneous branch of ulnar nerve.
VOLAR – Palmar cutaneous branch and digital cutaneous branches of the median nerve.
Relevant Anatomy:
Innervation
- Roots: C6, C7, C8.
- Nerve: Radial nerve.
- Sensory Territory: Dorsal radial aspect of the hand.
- Innervation Route: C6, C7, C8 → radial nerve → superficial branch of radial nerve.
Course: The radial nerve branches into the superficial branch and deep branch, also known as the posterior interosseous nerve, in the deep posterior proximal compartment of the forearm. The superficial branch continues distally and arises superficially between the brachioradialis tendon and the extensor carpi radialis longus tendon within the mid-forearm. Distally, the superficial branch innervates the dorsal radial aspect of the distal forearm/wrist and hand.