For reconstructions that include nerve autografts, there are available sources for donor nerves in the upper and lower extremity. The decision of which donor nerve to use depends on the case scenario and the patient’s needs during the pre-operative assessment. While sensory nerve graft harvests come at the sacrifice of the sensory territory, over time, these less-critical sensory territories can recovery some rudimentary sensation from adjacent functional sensory territories through collateral sprouting. To increase the potential for restoring rudimentary sensation to these territories, an end-to-side nerve transfer can be elected.
While sensory nerves have proven to be an excellent source for graft material, the surgeon needs to be aware of the anatomical and physiological differences between motor and sensory nerve fibers and consider expendable motor nerve grafts as an option. A nerve gap reconstruction with matched modality can enhance nerve regeneration as seen in experimental animal studies. While there are available sources for nerve grafts, there exist a small percentage of patients who have severe traumatic injuries where nerve autografts are not an option. In these cases, cadaveric allografts are utilized at the expense of immunosuppression.
Upper Extremity
Title: Medial Antebrachial Cutaneous Nerve Graft Harvest.
Published: 4/22/2011, Updated: 4/26/2011.
Author(s): Susan E. Mackinnon MD, Andrew Yee BS.
Division of Plastic and Reconstructive Surgery, Washington University School of Medicine, St. Louis, MO.
The medial antebrachial cutaneous (MABC) nerve is an available donor for nerve grafts and our institution’s preferred donor nerve graft for upper extremity nerve reconstructions. The MABC nerve is harvested from the medial aspect of the arm. Due to this location, only one extremity is required to be prepped for surgery as the MABC nerve can be harvested from the same arm as the nerve reconstruction. The MABC nerve originates from the medial cord, courses distal, and branches into an anterior and posterior branch. The anterior and/or posterior branch can be harvested depending on the length and diameter required for nerve reconstruction. An anatomical landmark used to easily identify the MABC nerve and its branches is the basilic vein, where the anterior branch is found anterior and the posterior branch is found posterior to this vein within the middle arm. Harvesting the MABC nerve will result in a sensory deficient in medial aspect of the forearm. To restore rudimentary sensation to the MABC nerve territory, the MABC nerve is end-to-side transferred to an adjacent functional sensory nerve. That is, the distal end of the transected donor sensory nerve is coaptated to the side of a sensory nerve through an epineurial window. The distal end of the donor MABC nerve can be end-to-side transferred to the sensory component of the median or ulnar nerve. If only the anterior branch is harvested, the distal end can be end-to-side transferred to the remaining posterior branch of the MABC nerve. In select cases, patients have reported full recovery of sensation with no sensory deficit in the MABC nerve territory following the end-to-side nerve transfer. The combination effects of the end-to-side nerve transfer and the spontaneous collateral sprouting from adjacent sensory territories could describe these outcomes.
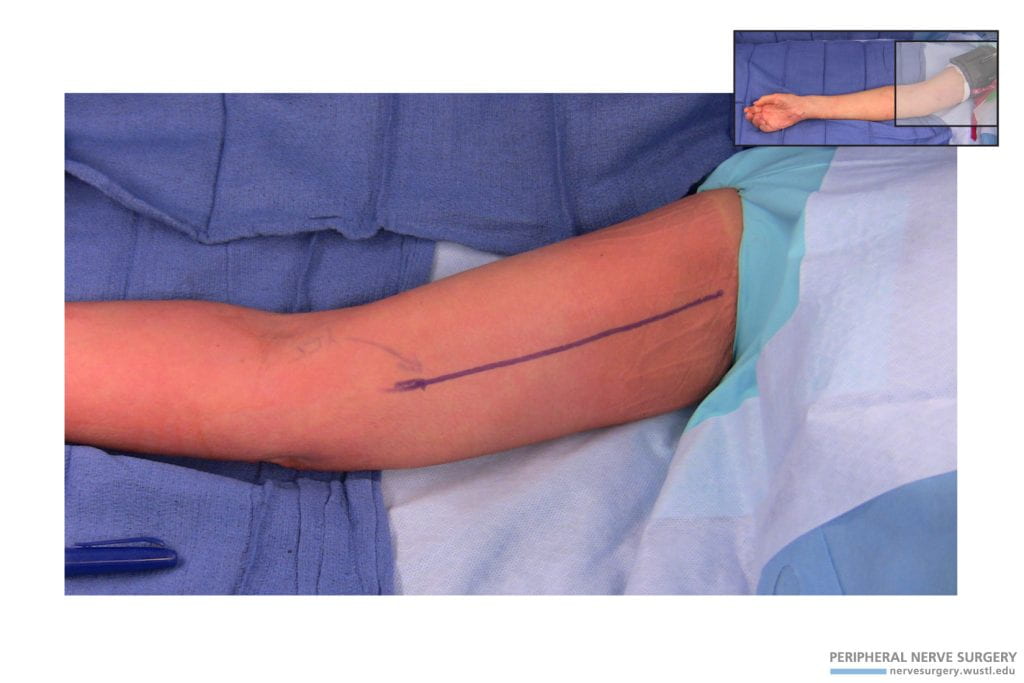
Figure 1 – Incision for Nerve Graft Harvest of the Medial Antebrachial Cutaneous Nerve. A longitudinal incision is made across the medial aspect of the arm with the patient supine.
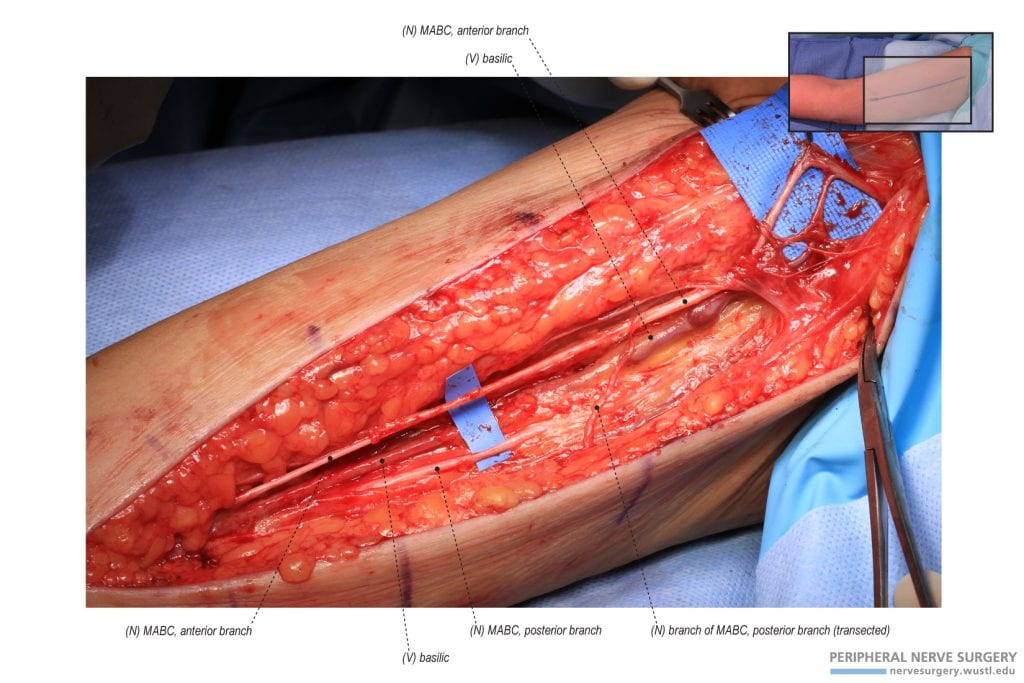
Figure 2 – Anatomy of the Medial Antebrachial Cutaneous Nerve During Surgical Exposure. The medial antebrachial cutaneous nerve is identified within the medial aspect of the arm. The MABC nerve originates from the medial cord, courses distal, and branches into an anterior branch and posterior branch. The basilic vein is an anatomical landmark to identify the MABC nerve. The anterior branch is found anterior and the posterior branch is found posterior to the basilic vein.
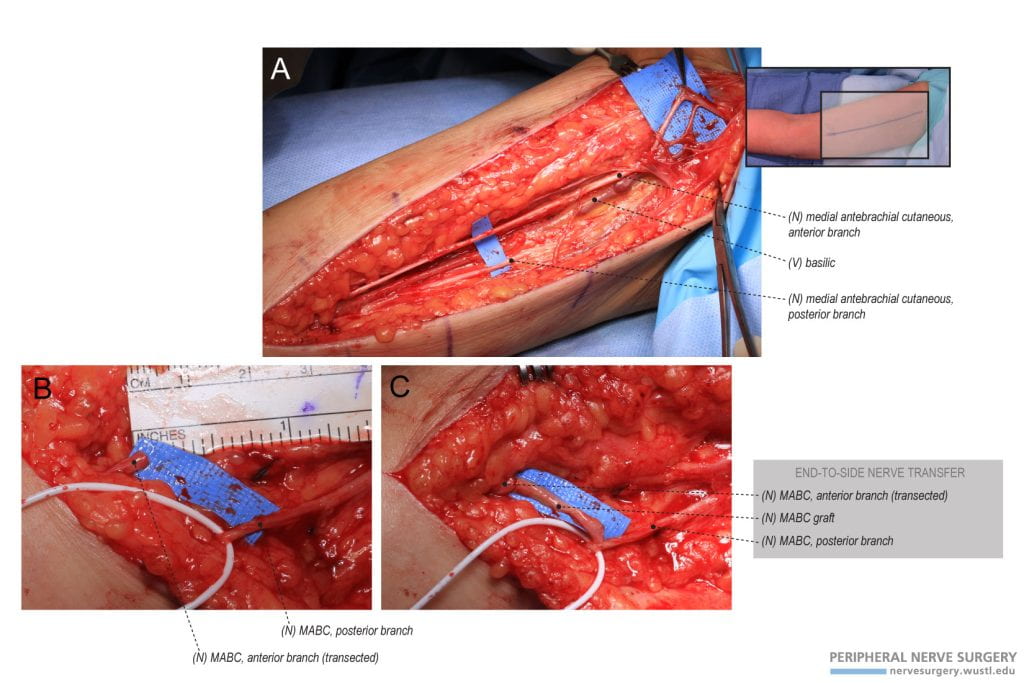
Figure 3 – Anterior Branch of Medial Antebrachial Cutaneous Nerve Graft Harvest. (A) The anterior branch of the medial antebrachial cutaneous nerve (MABC) was exposed superior to the basilic vein and isolated in the medial aspect of the arm. The posterior branch of the MABC nerve was also identified inferior to the basilic vein. (B) The anterior branch of the MABC nerve was harvested. (C) To restore rudimentary sensation in the MABC anterior branch distribution, the distal end of the MABC anterior branch was transferred to the MABC posterior branch in an end-to-side fashion. Following the prioritized ulnar nerve reconstruction with the harvested MABC graft, the unused MABC graft material was used to bridge the end-to-side nerve transfer for a tension-free repair.